Analysis Primer
A First Look At What’s Been Missing in Full Spine Analysis of Spinal Biomechanics.
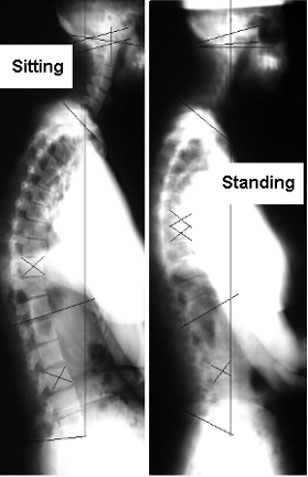
The full spine x-rays below were taken on the same patient, on the same day, with the patient standing relaxed letting their body slump and then sitting relaxed letting their body slump one minute apart.
There are enough changes of spinal configuration visible in this one set of films – changes which are not supposed to happen in minutes – to show most of the current chiropractic, medical, osteopathic, and physical therapy models of spinal motion and biostructural pathology are in need of some large modifications.
It is not so much that the models are incorrect as that the models are so rudimentary and lacking they have led to relatively ineffective treatment technologies.
Having the objective observations and the objective evaluations of treatment effectiveness that come with re-examination on standing and sitting full spine radiography leads to a much greater understanding of biomechanics. Having that improved understanding leads to improvements in biostructural treatments of the body such as chiropractic adjustments, for the first time allowing them to work consistently effectively with every patient. This does not mean it is magic and gets every one well immediately. It does mean the results are consistent and can be predicted. This is well beyond the dreams of most doctors. The fact that the results are generally much better than other methods is well beyond the dreams of most docs or what they have thought possible until now.
It was a long period between the discovery that mass is concentrated energy (Einstein’s E=mc2 which, in 1928 was initially called the biggest hoax in mathematics) and the development of the ability to utilize that data to create observable physical effects (atomic bombs and power plants) It has also been a long period between the discovery that abnormal body mechanics is the basic etiology of many neurological pathologies and syndromes and the development of consistently effective methods of biostructural treatment — those that will consistently and predictably correct the mechanical pathologies and reverse effects of those neurological pathologies and syndromes. Our time span has been a bit longer since there was no impetus of war to increase the funding and general effort of turning the data into usable treatment methods while there was and still is, a concerted effort by many who have a vested interest elsewhere to impede the development of effective physical methods of treatment. That is not a condemnation, just a statement of fact.
I am well aware of previous failed efforts to correlate postural vulgarities and other variations of physical position of the spine as measured on x-ray with neurological and musculoskeletal pathologies. (The spine is certainly not the only factor but it is where I started being a chiropractor.)
Though these previous researchers recorded their observations accurately they did not evaluate the data relative to the motion in the entire spine. They also did not evaluate the data relative to the function of the meninges as a mechanical stabilizer of the entire spinal column that instantly shifts mechanical stress throughout the column though this was specifically noted and published by the neurosurgeon Breig in articles and monographs starting before 1960.
Leaving out evaluation of the x-ray data relative to those factors and, missing observations during investigations (one such researcher stated a patient’s body had been not moved before rex-ray though stating the leg position of the patient was changed!) has led many doctors, therapists, anatomists and other researchers to misevaluate x-ray data relating to diagnosis and treatment of mechanical pathology as unreliable or useless. Many even call measuring body mechanics on full spine x-ray a hoax. This is strange since the x-rays are a factual picture of what is there at the time of the picture with known calculatable distortions. Some theories created from the observations are a bit funky (pardon the technical term there) but the x-rays and measurement of them are factual.
Evaluating the entire spine is a must for research on structural treatments because the spinal column works in a synchronized fashion. Every part instantly affects every other part. Doing evaluations of the ENTIRE SPINE in motion is a must for the same reason. Missing the synchronized workings of the entire spine has been the “hidden factor” blocking discovery of the basic mechanical pathology initiating musculoskeletal, neurological and even some organic pathologies that lead to dysfunction and pain. This is a fact the neurosurgeon Alf Breig described very specifically in 1978s.
Historically, Lhermitte and other researchers of the early 1900’s had postulated mechanical causes for neurological pathologies such as Multiple Sclerosis, ALS, and other “diseases” exhibiting similar neurological phenomena. In fact, all the physical orthopedic and neurological testing for these conditions are maneuvers attempting to increase the mechanical stresses creating the condition to evoke the signs associated with these conditions. As was stated by the neurosurgeon Ernest Sachs in 1949 “even some degenerative diseases of the nervous system, such as multiple sclerosis and the muscular dystrophies, may respond to surgical measures.”5 indicating mechanical factors were known even then.
The development of a method of biostructural treatment that consistently and predictably yields the results postulated by developers of various methods of biostructural treatment of disease has a history dating to ancient times just as the use of chemical compounds, herbs, and energy therapies such as acupuncture does.
Relatively recent breakthroughs leading to the development of consistent and predictably effective biostructural treatment are mostly due to two researchers, the neurosurgeon Dr. Alf Breig, author of Biomechanics of the Central Nervous System (1960), Adverse Mechanical Tension in the Central Nervous System (1978), and Skull Traction and Cervical Cord Injury (1989), and the chiropractor, Dr. Lowell Ward, author of The Dynamics of Spinal Stress (1977) and the Spinal Stressology Manual of Standard Practices (1986).
Dr. Breig’s contribution consists of the experiments leading to specific confirmation that the major mechanical factor precipitating these neurological conditions was axial tension (head to tail) on the spinal cord and brain stem (Central Nervous System). That tension was mostly precipitated by mechanical pathologies ranging from space occupying lesions to misalignment of the vertebrae which partially fixed the spinal column in flexion stretching the pons-cord tract.
In experiments and trails of therapy Dr. Breig noted the instant transmission of mechanical stress by the meninges along the entire spinal column and up into the skull. Those experiments laid the foundation explaining the mechanism by which pathologies and syndromes of the nervous system do not necessarily have their origin at the level of the spinal column or cord directly relating to the nerves affected but are originating as sequelae of mechanical misalignments (pathology).
Making that discovery and coming from a neurosurgical viewpoint, his solution was to develop the very effective Cervicolordodesis surgery. Cervicolordodesis is an operation that, using a plastic fastener to tie the head and neck back into a position of slight extension, slackens the pons-cord tract relaxing the tension on the central nervous system.
Breig’s research showed that “applying spinal cord relaxation it is possible to alleviate not only the neurological symptoms produced by outside forces on the pons-cord tract, but also those evoked by alteration of the cord tissue resulting from inflammation and reactive scar formation.” Note the statement is “by applying spinal cord relaxation” and not just using his surgical procedure. Though he did not delve into conservative treatments to discover the basic mechanical pathology which forced the spinal column into flexion, Breig did note that any approach truly relaxing the tension on the CNS would consistently and predictably alleviate the symptoms. In fact, he started his research into the positive effects of slackening the pons-cord tract and reducing axial tension on the central nervous system by using various outside the body mechanical methods of holding the patients’ heads in extension.
Breig’s direct experimentation and trails of therapy have led to the relief of the effects of cervical myelopathies, rhizopathies, trigeminal neuralgias, post-traumatic myelopathies, Multiple Sclerosis, Amyotrophic Lateral Sclerosis, Cerebral Palsies, urinary incontinence due to intra- and extramedulary lesions of various origins, and many more conditions previously not thought to be related to biomechanical pathologies.
Dr. Ward’s contribution came with the recognition that just as Breig noted the site of the mechanical lesion generating tension on the CNS could not be diagnosed without examining entire spine in flexion and extension, analysis and diagnosis of primary biomechanical pathologies (the basic misalignments for which other things compensate) in the spinal column-pelvis could not be diagnosed without examining the spinal column in multiple positions. Further, Ward noted the biomechanical stress patterns fixing patients’ spinal columns were most evident sitting but could not be diagnosed from single position examination due to the way other primary biomechanical pathologies in other regions of the spinal column affected compensation patterns. Mechanical pathologies can be precisely diagnosed by comparing sitting and standing biomechanical patterns noted radiographically though occasionally measurement of the body in additional positions is necessary for accurate diagnosis. (This confirmed Breig’s findings.)
Building upon the breakthroughs of these men, I have hypothesized and found consistent and predictable workability in analysis and clinical diagnosis and treatment the point that the basic mechanical pathology of the body is the movement, by any means, of a body structure into a position of decreased mechanical function from which the body cannot retrieve it. Think that through. Simple as it is it is the basic of mechanical pathology in the body. It says more than you might first realize.
Another point commonly noted but not accounted for in any mechanical theory is that the bones of the body work as a single mechanical mechanism levering the body upright. Like a set of interlocking gears, when one bone moves out of its optimal position it can no longer act as the lever it is. Therefore, with the bone misaligned the body begins to fall in the direction of lost leverage (later it will be demonstrated that, for reasons of mechanical design of the skeleton the direction a combination of forward right or left — actually a torque — and rarely posterior or posteriolateral.) The basic here is that an ideal body with bones in exactly the right position will stay upright with no muscular action. This is born out clinically. when people treated by these theories and mechanical analyses they stay upright with little or no effort and every function of the body has been measured to improve — thus the pictures at the opening of this web site.
As an example in the spinal column of the body not being able to move a bone in a direction needed for self-correction of structure: When a vertebra has become displaced anterior of its optimal position of function, there are no muscles or other motion inducing mechanisms that can pull that single vertebra in an anterior-to-posterior direction relative to the vertebrae above and below it with enough magnitude to reposition such a vertebra which has slipped or been forced anterior to its optimum position of mechanical function.
Experiments have been mentioned indicating that the various tissues attaching to the vertebrae will pull posterior when the body/spinal column is bent forward. However, like a rubber band held horizontal with a small weight at its center that can never completely be straightened by pulling at its ends, the physical reality is that the force anterior-to-posterior is not able to be exerted over enough distance to reposition the vertebra. (Those presenting the data on the posterior pull of these tissues neglect to notice the basic mechanics of the situation — that as the vertebra moves the angle of the tissues reduces and the force A-to-P reduces as a multiple function of the angle, ultimately not being enough to reposition the vertebra. They also miss the point that the other vertebrae are not any more stable than the one stuck forward, they are movable and get pulled out of position anteriorly as much as the vertebra stuck anterior is supposedly pulled posterior. the net result is no correction but compensation.)
Therefore, vertebrae in some way displaced with an anterior component of motion result in lost mechanical leverage holding the body upright. With the advantage of leverage gone, the body then must compensate for that loss. Compensating events ranging from the inconsequential to the enormously harmful occur resulting in most of the “disease” conditions described by Breig and others.
Most practitioners approach structural therapy with the presupposition that the body can move its parts in any direction and that the body is totally self-correcting. This is incorrect. For the body to self-correct/heal a very specific set of circumstances must be met. Consider a broken bone and how much effort must be taken to reposition and hold the position of the bone until it is substantially healed and what happens if it is not repositioned and held there.
Many believe the body only begins to mechanically malfunction when some component is damaged. They miss the small tolerances necessary for the most efficient and effective working of this complex a machine. They also miss the importance of instantaneous transmission of mechanical stress by the meninges and the fact of true interdependence of all motion in the body and, most importantly they miss the fact that bones and other structures can and do get moved in directions from which the body cannot retrieve them.
Other people do approach structural therapy with the presupposition that the condition presented can be a distant sequel to a mechanical pathology elsewhere. Those practitioners have the idea of slight changes in position causing large changes in function of the body and they have the thought of interdependence of motion (holism). However, they most often act and treat on a local effect basis because the theories on which their treatment is based have no specific cause consistently and predictably accounting for ALL the phenomena noticed in the body.
Via objective analysis of biomechanics using standing and sitting radiographs of the entire spine on one film or using two 14″x17″ sectionals shot at 72″ with the patient completely relaxed, the practitioner will find a consistent index and pattern of change in mechanics that can be used to determine the primary biomechanical pathology(ies) for which the compensations are generated, resulting in the various patterns of sequelae named as diseases. Knowing that data, appropriate application of biostructural treatments can be instituted. (This can now be done without x-ray.)
Nothing in this presentation should be interpreted to mean that manipulation of osseous structures is the only, treatment in these disorders. Depending upon the extent and intensity of the condition presented or permanent damages developed as sequelae to the mechanical pathology other biostructural therapies might be included to allow motion of the structures into their optimum positions or to provide the support needed for recovery. There is also the need to develop supports for those not able to fully recover to maintain and improve the extent of recovery available to all.
As Breig notes in his comment describing the sequence of improvements of neurological function in Cervicolordodesis patients (1), the traditional naming of neurological and spinal cord disorders “according to début, epidemiology, acute or chronic nature, etc., does not reflect the histodynamic causation of the symptoms.” That method of naming disorders has misled practitioners into thinking they have different etiologies. Breig further notes in that discussion, “It would be useful if the origin of the tension were stated in the diagnosis, for then the patient is more likely to receive the appropriate treatment.”
Below are films which demonstrate some of these changes and a basic explanation.
These are the films taken on the same person on the same day. The person is standing and sitting each picture is one minute apart. Note some changes on the laterals.
The pictures directly below are full size. If you want to print them just click on a photo and it will open up as the individual photo for you to print.
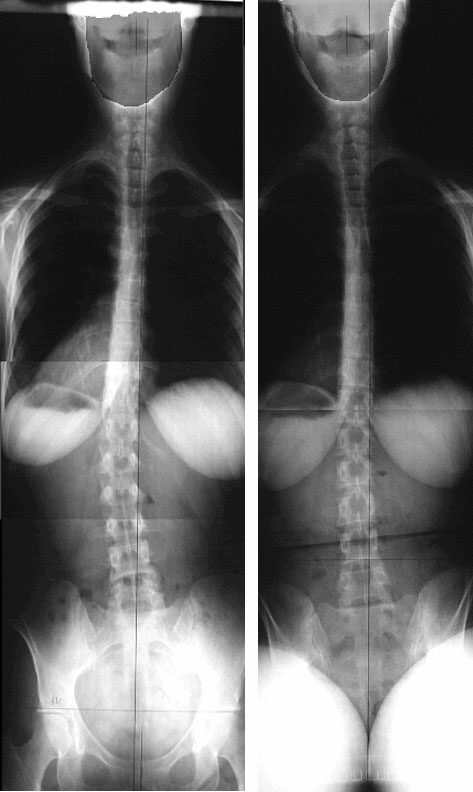
Most notable on the lateral view films above is that the cervical spine is military standing but becomes normally lordotic sitting. Also, the lumbar spine is in a hyperlordosis or sway-back standing and military/top half slightly reversed when sitting. These two curves are supposed to go in the same direction in a normal person. In this person, at the time of the x-rays, one is normal in the standing position or a bit more than normal, while the other is reversed. Sitting they switch but are still opposite. There is a compensation mechanism here in which they are working synchronously (changing instantly in concert with one-another)?
Which one do you treat? How do you treat it, and in which direction? Does it matter where the patient had pain? Should you treat at that point? Look below.
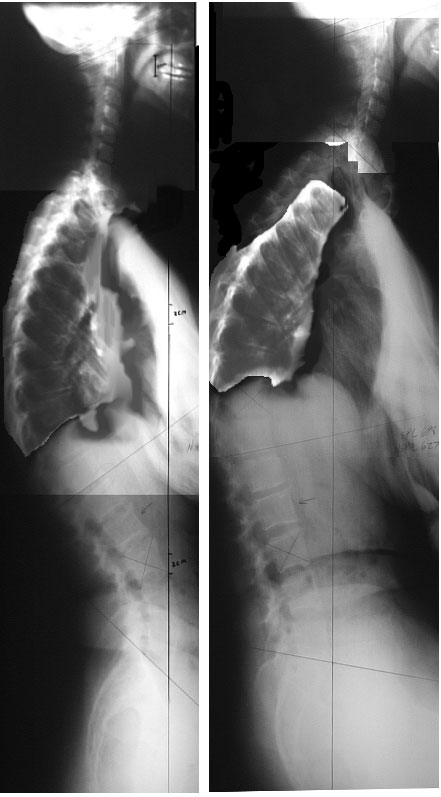
These are cutouts of the thoracic spines from the above films. The sitting thoracic section (middle) has been rotated 12 degrees counterclockwise so the curves can easily be compared.

How about the thoracic spine?
In this person the thoracic spine shows very little change from standing to sitting. It is easy to note that there are few significant changes from standing to sitting. All the changes are below the level of the apex of the kyphosis which is at T10 sitting and above T4 standing. (Apex = furthest point backward or forward in a curve. Important in analyzing the point of focus of mechanical stress.)
Also note that the mechanical leverage created by those changes in the thoracic spine, small as they are, account for the fact that the lumbar spine becomes hyperlordotic as the cervical spine loses its lordosis standing while the cervical spine is not forced to become hyperlordotic in compensation sitting when the lumbar spine loses its lordosis. Some of the increase in mechanical stress is taken up by the thoracics.
What about between T5 and the apex of the kyphosis when standing? The thoracic spine above T10 is not really a kyphosis. It just drops forward and would probably completely fold forward if it were not for the ribs. The ribs do not hold the thoracic spine rigid as so many biomechanical theories state they do. The ribs provide some support, but not stiffness to the point of rigidity. The thoracic spine has plenty of motion, especially in the AP direction.
The thoracic spine is a major compensator of biomechanical pathology and the most frequently injured portion of the column in P-to-A traumas such as automobile collisions.
That fact is not yet well documented or researched because not many doctors seem to notice. The reason might be that humans, in the standing position, use the large muscles attaching from the legs to the pelvis and spine to flex the pelvis and twist the lumbar spine into a hyperlordosis forcing the trunk backward to balance the collapsed thoracic spine. That makes the collapse of the thoracic spine less noticeable in the standing position as a biomechanical event because a pseudokyphosis is created by the compensation of the lower thoracic spine (canted posterior) and the portion of the thoracic spine above the standing apex falling anterior.
Why do the head and neck not fall anterior? They do but not completely. The effect of the meninges (Breig) and the leverage effect of the change in curve between the upper thoracic and cervical spine hold the neck and head up as much as possible just as the lumbars force the thorax posterior. What is often noted as normal is not even close to the optimum position. The variations from normal account for thoracic outlet syndrome including vascular and neurological signs as well as the many other symptoms and effects noted in this patient.
Common in the literature of radiology describing the various radiographic measurements of posture is the comment that such and such a range is normal. However, there is no specific correlation between findings outside of the range and symptomatology in the patient. The reason for this is stated at the outset of this presentation. The data of these measurements is not correlated with other mechanical data from the entire spinal column-pelvis to determine relative changes. With data from the entire spinal column-pelvis specific correlations between measurements and would quickly be determined.
The basic correlation is the determination of the lateral direction of that patient’s primary biomechanical pathology at that time.
The hypothesis for finding that, simply, follows this line. When standing, the body can arrange the bones of the lower extremities and use the contraction of the muscles of the lower extremities to twist the pelvis and spinal column into a compensated position.
When one sits with the feet flat on the floor before them, the use of the lower extremities and muscles are reduced. They cannot twist and pull enough to compensate as well so the collapse of the thoracic spine above a given point becomes more evident. Why say “more evident”? Shouldn’t the phrase just be evident? No, the collapse is noticeable standing if one knows what to look for.
After reading this you can probably find the flat spot in the lower thoracic curve (T12,11,10) above which the thoracic spine collapses even in the standing view. Go back to that film and check.
Comparing the standing film to the sitting one can predict the sites of pain via mechanical stress analysis and correlation of intensities with direction of mechanical stress. Also, the vertebrae in need of treatment can be determined since one can determine which are in flexion and unable to be repositioned by the body.
On the other hand, once one has x-rays comparing the pelvic tilts one can determine to which direction the body is falling due to inadequate bone leverage resulting from the biomechanical pathologies (people do stay upright because of muscle power but it is less necessary to use the muscles as the bones become more optimally positioned for leverage). Using that information, one can observe the body response to simple physical testing and determine which vertebrae to treat and which to ignore on any given day be they at the level of another type of pathology or not.
Important is that the segments malpositioned but not to be treated is determined. This is a vital determination because, though they may also be out of optimal position and may be at the site of mechanical stress causing other damage, those segments are out of position to compensate other malpositioned vertebrae and actually support the body. Changing their position can change their mechanical stress pattern of the body and relieve pain. However, that does not mean the patient’s condition is improved. Very often treatment of those areas results in an increased mechanical pathology with ot without precipitation of symptoms elsewhere in the body not — thought to be related.
This is also true of the patient in the films below who came into the office two days past. He had been treated by 9 other chiropractors, an osteopath, various types of massage therapies, all including posterior-to-anterior pressure on the thoracic spine. Pardon my abruptness but how is one to expect that thoracic spine or any thoracic spine to improve by being flattened further?
With the knowledge that many of those “hyperkyphosis” are actually the thoracic spine pathologically falling forward over a leverage point, P-to-A pressure on the thoracic spine should be discarded as a therapy. This miscalculation, among others even more significant but less obvious, have kept biostructural therapies from being effective with every patient that presents for treatment.
References
1. Breig, A.: Biomechanics of the Central Nervous System 1960, Almqvist, Stockholm
2. Breig, A.: Adverse Mechanical Tension in the Central Nervous System 1978, Almqvist, Stockholm
3. Breig, A.: Skull Traction and Cervical Cord Injury 1989, Almqvist, Stockholm
4. Kabat, H.: Low Back and Leg Pain From a Herniated Cervical Disc 1980, Green, St. Louis
5. Sachs, E.: Diagnosis and treatment of brain tumors and care of the neurosurgical patient. 2 Ed. Mosby, St. Louis, IL 1949.
6. Ward, L.: The Dynamics of Spinal Stress 1980, Long Beach, CA.
7. Yochum T, Rowe L,: Essential of Skeletal Radiology 1986, Williams, Baltimore.

Three of these pictures have the extravertebral area darkened for better viewing. The configurations are unaltered. These pictures are not very clear for faster loading of this page. If you right click on the picture and click open in another window, you can get a more clear view. Do it for each picture pair and place them side by side. You can also print them out and look at the hard copy which will have better resolution.
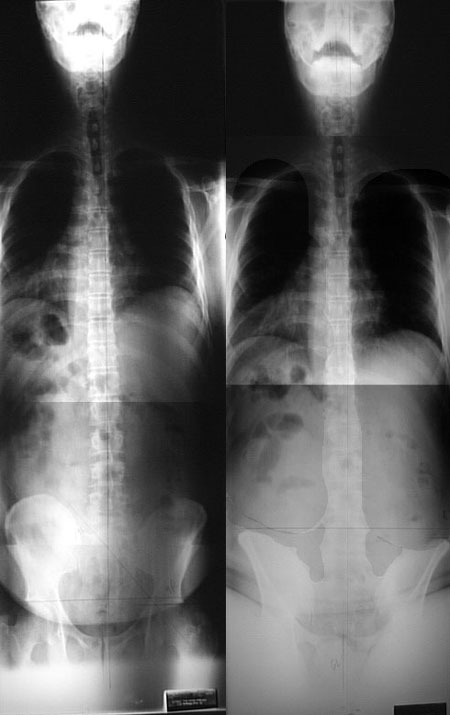
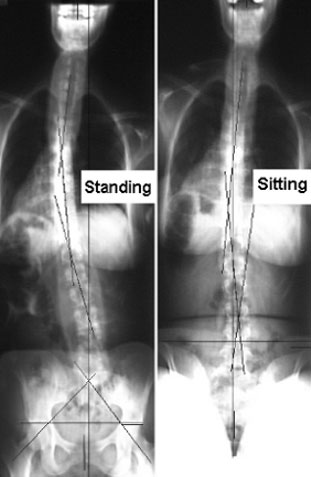
Now it’s your turn. These are a set of full spine standing and sitting laterals and AP’s taken of a young lady within four minutes. What is the direction of her main biomechanical pathology?
Think in three dimensions. Is her main biomechanical pathology that she is twisted anterior-left, posterior-left, anterior-right, posterior-right? Would you adjust this woman’s thoracic spine P-to-A? Is that lumbar scoliosis a biomechanical pathology (subluxation complex) to be concerned about? Is it a compensation that will quickly disappear when you start to correct the main pathology? What about the thoracic scoliosis? Why does her cervical lordosis disappear when she stands?
Her complaint was neck pain and headaches. She was scheduled for TMJ surgery four weeks from her first visit to our office because she could not open her mouth more than half the width of her thumb.
What would you do if you only had standing laterals of the area of pain, her cervical spine? Do you know how to handle people with managed care?
Write up your analysis on a sheet of paper. Fax it to me at the number above or mail it,
I will reply.